This
post was originally published on
this sitehttp://chriskresser.com/

Vitamin D is critical for health. Virtually every cell in the body has a vitamin D receptor, which, when bound to vitamin D, can influence the expression of more than 200 genes (1, 2). Vitamin D promotes calcium absorption in the intestine and maintains calcium and phosphate levels in the blood, protecting against osteoporosis, rickets, and bone fracture (3, 4). It also regulates immune function, cell growth, and neuromuscular function (5, 6).
With the many roles that vitamin D plays in the body, deficiency of this fat-soluble vitamin is a real cause for concern. Vitamin D deficiency has been found to increase the risk of heart attack, cancer, diabetes, asthma, and autoimmune disease (7, 8, 9, 10, 11, 12). Our modern indoor lifestyle limits our sun exposure, and we can only get a small amount of vitamin D from diet (13). According to the lower boundary of the U.S. lab range of 30 ng/mL, as many as 70 percent of Americans are considered deficient (14, 15).
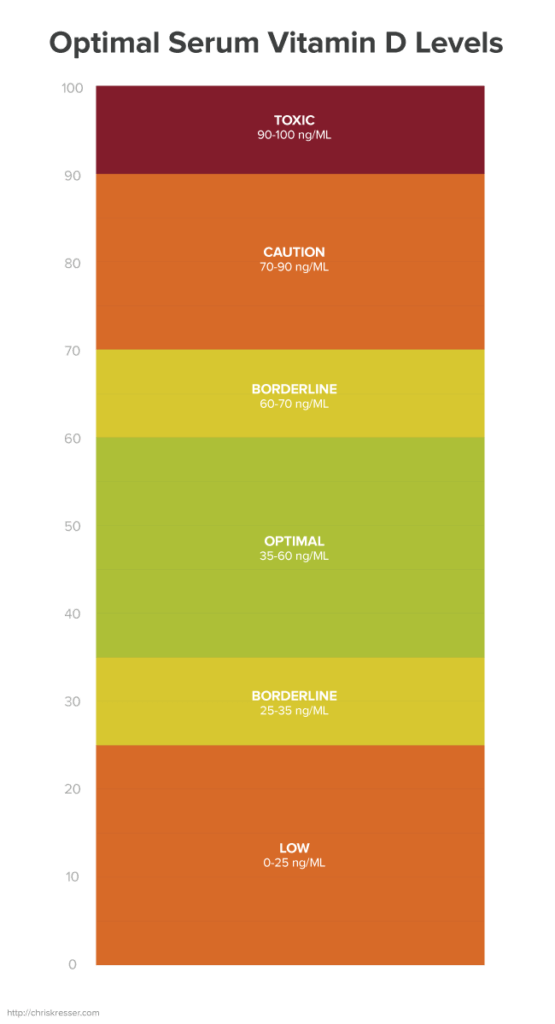
It’s great that awareness about vitamin D deficiency is increasing, with more doctors than ever testing vitamin D levels. However, like many nutrients, vitamin D follows a U-shaped curve, meaning that both low levels and very high levels are associated with negative health outcomes (16). Unfortunately, few practitioners are aware of the dangers of vitamin D toxicity, and many just test serum vitamin D once and recommend a daily 5,000 or 10,000 IU supplement to their patients.
In this article, I’ll discuss the risks of over-supplementation, why you should get most of your vitamin D from sunlight, and the reasoning behind my current approach to vitamin D.
Risks of excess vitamin D supplementation
Vitamin D status is measured by 25(OH)D in blood. We’ll dive further into vitamin D metabolism later, but for now, just understand that this is the precursor to active vitamin D and is generally considered the most accurate single marker to assess vitamin D status. The U.S. laboratory reference range for adequate 25(OH)D is 30 to 74 ng/mL, while the Vitamin D Council suggests a higher range of 40 to 80 ng/mL, with a target of 50 ng/mL (17).
But a large body of evidence in the medical literature strongly suggests that optimal vitamin D levels might be lower than these figures. There is little to no evidence showing benefit to 25(OH)D levels above 50 ng/mL, and increasing evidence to suggest that levels of this magnitude may cause harm. Consequences of vitamin D toxicity include heart attack, stroke, kidney stones, headache, nausea, vomiting, diarrhea, anorexia, weight loss, and low bone density (18).
Furthermore, in most studies, taking vitamin D supplements does not decrease risk of death, cardiovascular disease, or other conditions. Based on an exhaustive review of over 1,000 studies in 2011, the Institute of Medicine recommends a much more conservative range of 20 to 50 ng/mL (19).
Some research on Israeli lifeguards suggests that, contrary to popular belief, vitamin D toxicity from sunlight alone (in the absence of supplementation) is possible (20). That said, it is much more difficult to achieve toxic levels through sun exposure alone. Sunlight is the optimal source of vitamin D, and has numerous benefits above and beyond improving vitamin D status.
Beyond vitamin D: The many benefits of sunlight
Vitamin D is really just the tip of the iceberg when it comes to the benefits of sunlight. A recent 20-year study following 29,518 subjects found that those individuals avoiding sun exposure were twice as likely to die from all causes (21). While this study did not assess vitamin D levels, findings from other epidemiological studies suggest that this cannot be accounted for by the increase in vitamin D production alone.
Indeed, humans make several important peptide and hormone “photoproducts” when our skin is exposed to the UVB wavelength of sunlight (22). These include:
- β-Endorphin: a natural opiate that induces relaxation and increases pain tolerance (23, 24)
- Calcitonin Gene-Related Peptide: a vasodilator that protects against hypertension, vascular inflammation, and oxidative stress (25)
- Substance P: a neuropeptide that promotes blood flow and regulates the immune system in response to acute stressors (26)
- Adrenocorticotropic Hormone: a polypeptide hormone that controls cortisol release by the adrenal glands, thus regulating the immune system and inflammation (27)
- Melanocyte-Stimulating Hormone: a polypeptide hormone that reduces appetite, increases libido, and is also responsible for increased skin pigmentation (27)
Exposure to the UVA wavelength of sunlight has also been shown to have benefits, including increasing the release of nitric oxide from storage (28). Nitric oxide is a potent cellular signaling molecule that dilates the blood vessels and thus reduces blood pressure (29).
In addition to the production of photoproducts and release of nitric oxide, sunlight also entrains circadian rhythms. Exposure to bright light during the day activates neurons in the suprachiasmatic nucleus of the hypothalamus, which sends signals to the pineal gland that regulate melatonin production. Disruption of circadian rhythm has been associated with mood disorders, cognitive deficits, and metabolic syndrome (30, 31).
Optimal vitamin D range depends on many factors
So how much do you need? At the first annual IHH-UCSF Paleo Symposium in San Francisco this year, nutritional biochemist Dr. Chris Masterjohn summarized evidence suggesting that optimal vitamin D levels may vary from population to population, despite the fact that there is currently only one reference range used for all patients.
Ethnicity is one major consideration. For example, blacks have lower 25(OH)D than whites in the U.S., yet they typically have much higher bone mineral density. Furthermore, non-Caucasians have lower 25(OH)D levels than Caucasians, even at their ancestral latitudes (32). From these and other studies, it has been suggested that people with non-white ancestry may be adapted to a lower optimal 25(OH)D level than people with white ancestry.
Another factor that influences toxicity is nutritional status. The fat-soluble vitamins A, D, and K work synergistically, and adequate vitamin A and K may protect against toxic effects of excess vitamin D (33). Sufficient levels of potassium and magnesium have also been suggested to protect against vitamin D toxicity (34). Unfortunately, most people are deficient in these micronutrients in the developed world, making them more susceptible to vitamin D toxicity.
What about optimal vitamin D range from an evolutionary perspective? A study on traditionally living hunter–gatherer populations in East Africa found that the Masai and Hadzabe tribes had average 25(OH)D concentrations of 48 ng/mL and 44 ng/mL, respectively (35). These indigenous populations get a great deal of sun exposure but also have very high intakes of vitamins A and K, suggesting that these levels are probably towards the higher end of the optimal range for most people in the modern world.
Using parathyroid hormone levels to individualize vitamin D testing
As we saw in the last section, 25(OH)D lab ranges should vary by population, genetics, and nutritional status. In the absence of specific ranges, we need other biological markers that can help to clarify vitamin D status. To find these biological markers, we need to look at how vitamin D is metabolized.
When UVB contacts the skin epidermis, vitamin D is produced from 7-dehydrocholesterol. This vitamin D then travels in the blood to the liver, where it undergoes primary hydroxylation (the addition of a hydroxyl group, consisting of one oxygen and one hydrogen atom) on the 25th carbon atom. The result is 25(OH)D, which is the metabolite most widely used to assess nutritional vitamin D status. This compound circulates in the blood until it undergoes secondary hydroxylation on the first carbon atom in the kidney, resulting in 1,25(OH)2D, the active form of vitamin D (36).
You might be wondering: why don’t we test the active form? While certainly informative, the amount of active vitamin D is not directly reflective of nutritional vitamin D status because the secondary hydroxylation step is tightly regulated by parathyroid hormone (37). When the parathyroid glands sense a drop of blood calcium levels, they secrete parathyroid hormone (PTH). PTH stimulates the formation of active vitamin D, which increases calcium absorption in the small intestine and calcium release from bone in an attempt to restore normal blood calcium levels (38). High PTH levels can therefore lead to high 1,25(OH)2D, low bone mineral density, increased risk of fractures, and osteoporosis (39).
With a basic understanding of this pathway, we can use PTH, calcium, and active vitamin D3 as markers to give us a more complete picture of someone’s vitamin D status. In his presentation at IHH-UCSF, Dr. Masterjohn suggested that serum PTH levels above 30 pg/mL may be indicative of biological vitamin D deficiency when 25(OH)D levels are borderline low. Conversely, if 25(OH)D levels are borderline low or even slightly below the laboratory reference range (e.g., 25 to 30 ng/mL), but PTH is less than 30 pg/mL, it is unlikely that the patient is vitamin D deficient, and supplementation is not warranted.
Instead of focusing on the 25(OH)D level itself, what we really want to achieve is maximum suppression of PTH levels for optimal calcium homeostasis and bone health. Beyond this level, more vitamin D is not necessarily better.
Conclusion
Based on my assessment of the literature and my own clinical experience, I believe the functional range for 25(OH)D is around 35 to 60 ng/mL. However, I can’t stress enough that there is significant variation among populations. For those with non-white ancestry, the optimal range may be a bit lower. For those with autoimmune disease, the optimal range might be a bit higher (45 to 60 ng/mL) to maximize the immune-regulating benefits of vitamin D. Here are a few recommendations for optimizing your vitamin D level.
- Don’t supplement blindly.
If your 25(OH)D level is:
- less than 20 ng/mL: you likely need some combination of UV exposure, cod liver oil, and a vitamin D supplement
- 20 to 35 ng/mL: get your PTH tested. If PTH is adequately suppressed (less than 30 pg/mL), supplementing is probably unnecessary.
- 35 to 50 ng/mL: continue your current diet and lifestyle for maintaining adequate vitamin D
- greater than 50 ng/mL: try reducing your vitamin D supplements, and make sure you are getting adequate amounts of the other fat-soluble vitamins to protect against toxicity
- Get retested!
Check your levels after three to four months to see if you have achieved or maintained adequate levels of vitamin D. If not, adjust your diet, lifestyle, or supplements accordingly and check again in another three to four months.
- Get sunlight or UV exposure as your primary form of vitamin D.
Reap the many benefits of sunlight beyond just subcutaneous production of vitamin D, and reduce your chance of achieving toxic levels. Spend about 15 to 30 minutes, or about half the time it takes your skin to turn pink, in direct sunlight. Sunscreens not only block production of vitamin D, but also all of the other beneficial photoproducts produced in the skin in response to UVB.
- Mind your micronutrients to protect against toxicity.
Try cod liver oil as a good source of vitamins A and D and high-vitamin butter oil or pastured butter and ghee for vitamin K. Sweet potatoes, bananas, plantains, and avocados all contain significant amounts of potassium. Consider supplementing with magnesium as it is very difficult to get adequate amounts of this micronutrient from food due to soil depletion.
Now I’d like to hear from you. How often do you get your vitamin D levels tested? Do you take a supplement? Have you ever had your PTH levels tested? Let us know in the comments!






 For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>
For now classes are 6pm and 640pm at 2840 Wildwood st in the Boise Cloggers studio.
Book your class NOW!
click this ==>







